FISTULA TREATMENT
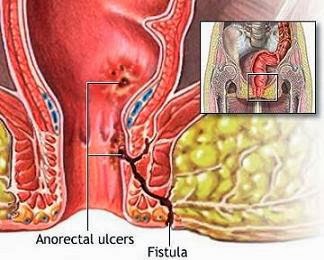
The goals of treatment of a fistula-in-ano are the elimination of sepsis and of the fistula tract, the prevention of recurrence, and the preservation of continence. A fistula-in-ano always traverses or passes through a portion of the internal anal sphincter and usually some, if not all, of the external anal sphincter.
Treatment of an anal fistula requires surgery in an operating room under general or regional anesthesia. The majority of fistulae can be managed by simply laying open the fistula tract. This involves dividing the overlying tissue, which includes a portion of the sphincter complex. The chronic inflammatory tissue is removed and the wound is allowed to heal secondarily by scar tissue formation.
For fistulas that involve the internal anal sphincter or only a small portion of the external anal sphincter there is a small risk of incontinence postoperatively. The greater the amount of external sphincter traversed by the fistula, the greater the risk of postoperative incontinence after the lay-open technique.
Alternative treatments are available for persons in whom the risk of incontinence would be too great using this technique. The most commonly used method is the use of a seton.
A seton is a thread passed around the fistula tract. It can be made of many different materials including silk or nylon suture, rubber, or plastic. Setons can be used in many different ways. They can act as drains to prevent recurrent infections. They can mark the site of a fistula tract to permit it to be divided in stages, thus reducing the chance of postoperative incontinence. Finally, they can be intermittently tightened to slowly cut through the sphincter muscles. The rationale here is that healing and scarring occurs as the seton cuts through the muscle, preventing division of the muscle all at once.
For a patient with a fistula that is not amenable to either the lay-open technique or treatment with a seton, there are a number of more complex surgical procedures available. The most commonly used is the creation of a flap of tissue in the anal canal to cover the internal opening in combination with drainage of the external opening and fistula tract.
The type of surgery will depend on the position of your anal fistula. The options include:
- Fistulotomy. This is used in 85-95% of cases and involves cutting open the whole length of the fistula in order for the surgeon to flush out the contents. This heals after one to two months into a flattened scar.
- Seton techniques. A seton is a piece of thread which is left in the fistula tract. This may be considered if you are at high risk of developing incontinence when the fistula crosses the sphincter muscles. Sometimes several operations are necessary
- Advancement flap procedures. This option is usually when the fistula is considered complex, or is there is a high risk of incontinence. The advancement flap is a piece of tissue that is removed from the rectum or from the skin around the anus. During surgery, the fistula tract is removed and the flap is reattached where the opening of the fistula was. The operation is effective in about 70% of cases. Fibrin glue. This is currently the only non-surgical treatment option. The glue is injected into the fistula to seal the tract, then the opening is stitched closed. It is a simple, safe and painless procedure, but long term results for this method are poor. Initial success rates as high as 77% drop to 14% after 16 months.
- Bioprosthetic plug. This is a cone shaped plug made from human tissue, which is used to block the internal opening of the fistula. Stitches keep it in place. However, this does not completely seal the fistula, so that it can continue to drain. New tissue usually grows around the plug to heal the fistula. Two trials show success rates of over 80% for this method, but long term success rates are uncertain.
Make an Appointment